Semax
•Synthetic heptapeptide analog of ACTH(4–10).
•Developed in Russia and mainly studied for:
•cognitive effects
•neuroprotection
•Most published clinical literature uses intranasal administration, but some research discussions reference subcutaneous (SC) routes as a once-daily alternative.
Educational research dosing concepts (preclinical / non-human discussions)
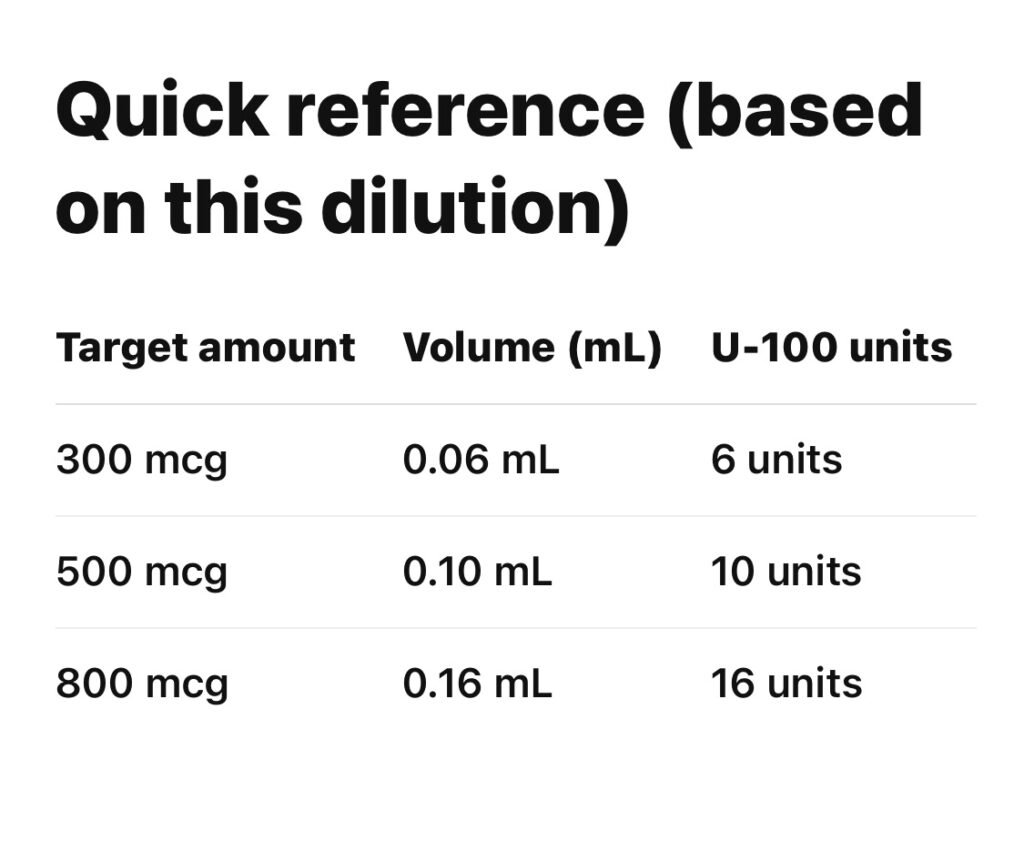
•Common referenced daily range: 300–800 mcg
•Typically introduced at lower amounts first.
•Gradual titration is often described in research contexts.
⸻
Reconstitution (educational reference)
•Vial content: 10 mg Semax
•Add: 2.0 mL bacteriostatic water (BAC water)
General lab handling concepts:
•Use sterile technique.
•Slowly add diluent down vial wall.
•Allow peptide to dissolve fully (≈20 minutes mentioned).
•Avoid aggressive shaking.
Concentration after reconstitution
Let’s calculate:
Step 1 — Convert mg to mcg
•10 mg = 10,000 mcg
Step 2 — Divide by total volume
10{,}000 \text{ mcg} \div 2.0 \text{ mL} = 5{,}000 \text{ mcg/mL}
Final concentration:
5,000 mcg per mL
U-100 insulin syringe reference
Key fact:
•U-100 insulin syringe = 100 units = 1.0 mL
So:
•1 unit = 0.01 mL
•10 units = 0.1 mL
•50 units = 0.5 mL
For example:
500 mcg = 0.1 mL
On a U-100 insulin syringe:
0.1 mL = 10 units (the “10” mark)
Important educational safety notes
•Published human clinical protocols primarily involve intranasal use; SC use is less standardized in literature.
•Research peptide purity, stability, and sterility can vary widely.
•Handling peptides or injections outside controlled lab or veterinary settings carries risks (dosing error, contamination, tissue injury).