Sermorelin is a synthetic analog of growth hormone–releasing hormone (GHRH). It stimulates the pituitary to release endogenous growth hormone, which may increase downstream IGF-1 levels. It was historically FDA-approved for pediatric GH deficiency but is commonly discussed in research contexts for adult GH support.
Typical research descriptions emphasize:
 Mimicking natural physiology by stimulating GH release rather than replacing GH directly
Mimicking natural physiology by stimulating GH release rather than replacing GH directly
Once-daily subcutaneous administration
Bedtime dosing to align with natural nocturnal GH pulses (peak secretion occurs during sleep)
Important context:
•Many products marketed today are labeled research use only and are not FDA-approved medications.
•Protocols vary widely in research literature.
⸻
Reconstitution (educational reference)
Given:
•Vial: 10 mg Sermorelin (lyophilized powder)
•Diluent: 2.0 mL bacteriostatic water (BAC water)
•Syringe: U-100 insulin syringe (100 units = 1 mL)
Step overview (general sterile research handling)
1.Add 2.0 mL BAC water slowly into the vial.
2.Aim the stream against the vial wall to reduce foaming.
3.Gently swirl — do NOT shake vigorously.
4.Allow ~15–20 minutes for full dissolution.
⸻
Resulting concentration (key math)
Total drug = 10 mg
Total volume = 2 mL
 Concentration:
Concentration:
5 mg/mL
or
5000 mcg/mL
⸻
U-100 syringe conversion
A U-100 insulin syringe:
•100 units = 1 mL
•1 unit = 0.01 mL
Now convert:
5000 mcg per 1 mL
50 mcg per 1 unit
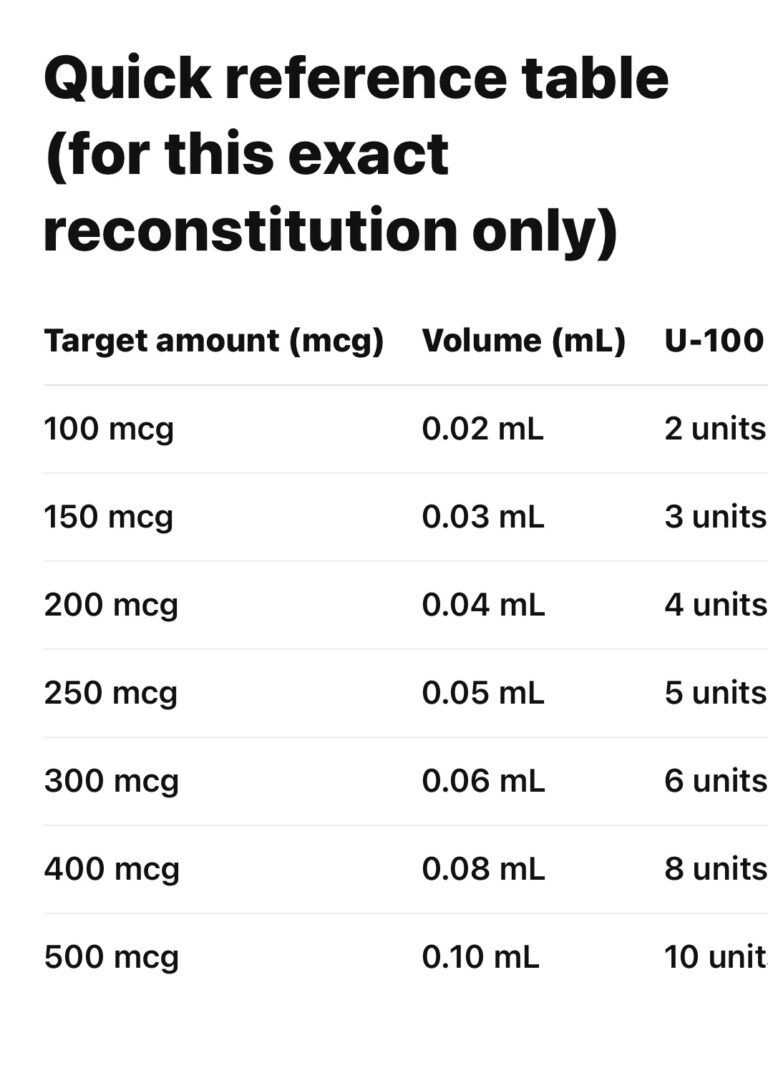
Simple rule for this specific mixture:
1 unit on the syringe = 50 mcg Sermorelin